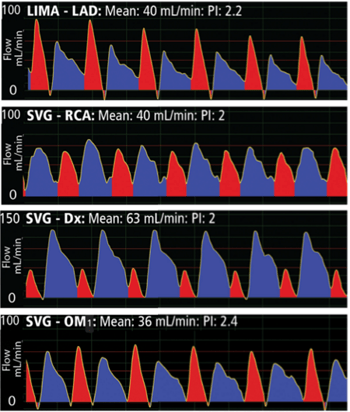
 Analysis of a flow waveform is useful when the mean flow of the bypass graft is questionable, between 5 mL/min and 20 mL/min. But what should one look for? First, the waveform should have a smooth, repeatable flow profile. Secondly, there generally should be clear definition of a biphasic waveform representing systole and diastole as shown in the following example of four patent grafts in an 83-year-old patient.
Analysis of a flow waveform is useful when the mean flow of the bypass graft is questionable, between 5 mL/min and 20 mL/min. But what should one look for? First, the waveform should have a smooth, repeatable flow profile. Secondly, there generally should be clear definition of a biphasic waveform representing systole and diastole as shown in the following example of four patent grafts in an 83-year-old patient.
However, waveforms can differ considerably depending on the following:
- The source of flow, or how far down the aorta is the proximal anastomosis of the graft. Pressure, the driving force behind the flow, changes as it moves down the arterial tree.
- The mechanical properties of the graft: An artery exhibits more elasticity than a vein and will expand in order to store blood released during systole. Flow measured at the base (proximal end) of an arterial bypass will have a stronger systolic component than flow at the distal end because of this systolic filling phenomenon. A vein bypass exhibits less of this phenomenon.
- The target site of the bypass graft: During systole, the heart muscle contracts and does not accept flow. Atria contract before ventricles, so the timing of the no-flow period varies depending on the target site to which the bypass is grafted.
- The condition of the target vasculature: If the target cardiac vasculature is severely diseased, it will exhibit a higher resistance to flow. This will likely be expressed as a less pronounced difference in flow resistance between systole and diastole (flatter curves) and lower average flow.
- Peripheral conditions, such as:
- An arterial bypass can go into spasm and alter flow.
- Competitive flow from the native coronary.
- A bypass graft can be anastomosed to the heart so it not only supplies blood to a target vasculature of disease heart muscle but also to a larger area of the coronary tree (collateral flow).
- Individual patient systolic/diastolic blood pressure levels.
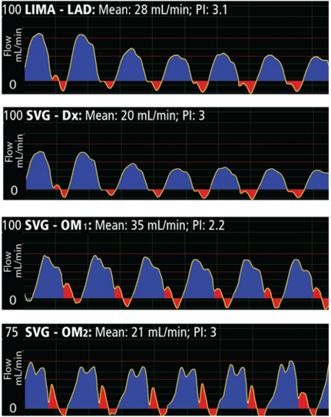
The waveforms below demonstrate unusual profiles with strong diastolic components in all the waveforms, but with almost no systolic flow in the left heart LIMA-LAD and SVG-Dx grafts and small systole in the right heart OM1, OM2 grafts. This is most often due to sub-myocardial coronaries, and, if mean flow is adequate, has no bearing on anastomotic quality of the grafts.